| Drug Name | ROD-16 |
| Description |
ROD-16 is a next-generation oxalate decarboxylase in phase II clinical development for the oral treatment of secondary hyperoxaluria. Partial phase II data showed higher efficacy of ROD-16 with a favorable safety profile consistent with other oral enzymes. Phase I clinical trials are also ongoing in patients with primary hyperoxaluria or nephrolithiasis. ROD-16 is expected to treat primary and secondary hyperoxaluria as well as nephrolithiasis. |
| Drug Modality | Recombinant protein |
| Indication | Hyperoxaluria |
| Product Category | Enzyme |
| Mechanism of Action | Degrading oxalate in the upper gastrointestinal tract |
| Status | Phase II |
| Patent | Granted |
Protheragen Inc. is actively seeking partnership for ROD-16. Potential collaboration can be strategic alliance, licensing, or marketing agreement.
We look forward to hearing from you.
ROD-16 is an orally administered oxalate-specific enzyme that is designed to effectively degrade oxalate to natural byproducts in the upper gastrointestinal (GI) tract. ROD-16 is produced by recombinant expression in T. reesei. Due to its high-potency composition and unique level of stability in the upper GI tract, ROD-16 does not require a threshold oxalate level for activity.
Hyperoxaluria is an important contributor to nephrolithiasis. According to the cause of excessive oxalate in urine, it is divided into primary and secondary hyperoxaluria. Primary hyperoxaluria is caused by an inherent genetic defect or lack of specific enzyme activity, which eventually leads to significantly elevated levels of oxalate in the body. The causes of secondary hyperoxaluria include increased dietary ingestion of oxalate, intestinal pathologies, or changes in intestinal microflora. Both primary and secondary hyperoxaluria can present with kidney stones, and even relatively small changes in urinary oxalate can have a very significant impact on kidney stone formation. In addition, the presence of hyperoxaluria alone without concurrent nephrolithiasis can also have deleterious effects on the kidney, leading to fibrosis, acute kidney injury, and tubular atrophy.
Epidemiologic data show that the prevalence of hyperoxaluria ranges from 1 to 3 cases per 1 million population in the United States, with an approximate incidence rate of approximately 1 case per 58,000 population worldwide. The rates of hyperoxaluria are typically higher in Asian countries than in Western countries. Treatment of patients with hyperoxaluria includes conservative medical and surgical measures, as well as treatment of nephrolithiasis.
Oxalate is derived from a variety of dietary and endogenous sources and is an end product of human metabolism. Under normal circumstances, the majority of urine oxalate is derived from endogenous hepatic production. Any oxalate absorbed from the diet or produced endogenously is delivered to the kidney, where it is freely filtered and excreted as urinary oxalate. An increase in oxalate gastrointestinal absorption or hepatic oxalate production increases plasma and urinary oxalate, contributing to the risk of stone formation and other adverse renal disorders.
Oral administration of oxalate decarboxylase (OxDC) to enzymatically degrade oxalate in the gastrointestinal tract is a novel potential therapeutic strategy. OxDC is a Mn-dependent hexameric enzyme derived from Bacillus subtilis. It cleaves the carbon-carbon bond of oxalate to carbon dioxide and formate through a radical based catalytic cycle involving electron transfer from the coordinated Mn2+ ion to bound oxygen in domain I of each monomer. ROD-16 is a novel recombinant OxDC designed to efficiently degrade oxalate in the upper gastrointestinal tract. Compared to wild-type OxDC, ROD-16 has higher activity, greater stability in the upper gastrointestinal tract, and no requirement for an oxalate level threshold.
Phase I clinical trial has been completed and the phase II is ongoing. All pre-determined endpoints in healthy volunteers were met. Partly completed phase II clinical data demonstrated the high efficacy of ROD-16.

|
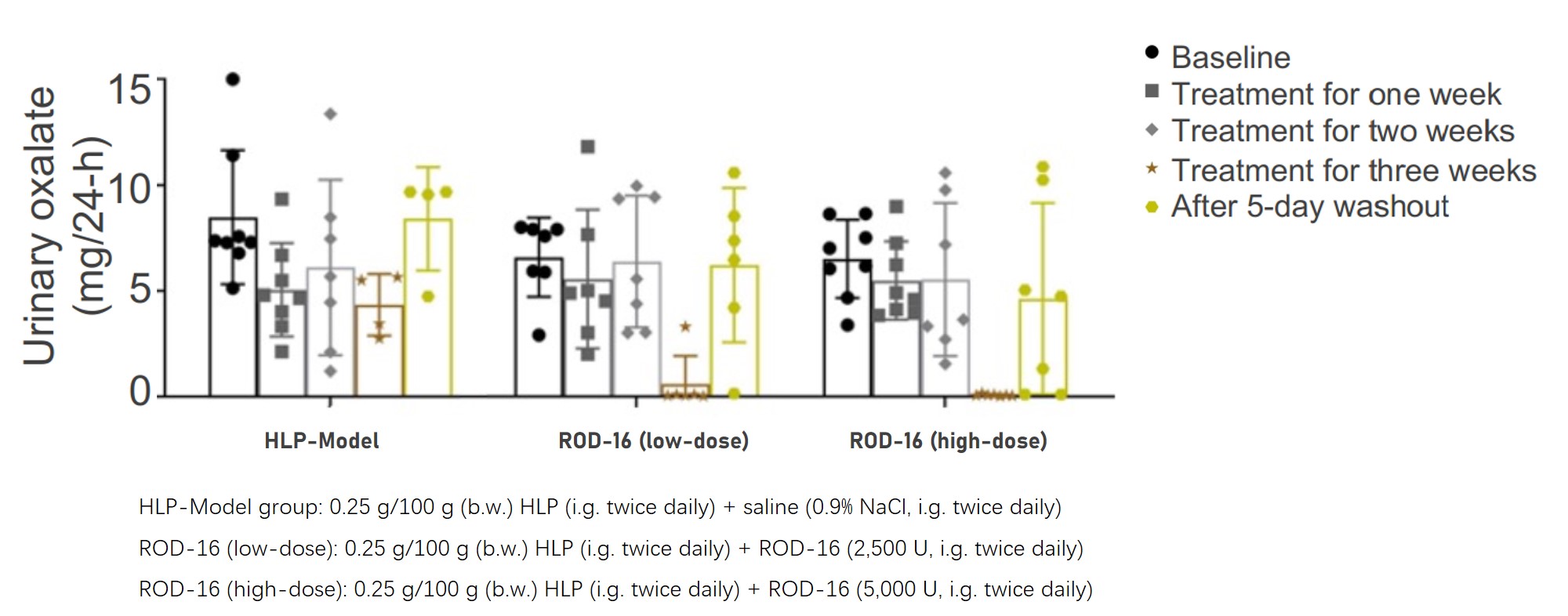
A Rat Model of Hyperoxaluric Calcium Oxalate Nephrolithiasis Induced by Hydroxy-L-prolineHydroxy-L-proline (HLP) is an oxalate precursor found in various diets. It has been shown to induce overproduction of endogenous oxalate and CaOx crystal formation in rodents. After 3 weeks of treatment with ROD-16, the 24-hour urinary oxalate of rats with primary hyperoxaluria induced by HLP dropped to almost 0. |
Protheragen's business is growing rapidly after founded in New York. Our business has evolved from the initial cross-border BD consulting service to encompass segments in equity investment and project incubation.
 |
Protheragen Inc. |
 |
Quick Links |